Laparoscopic sleeve gastrectomy( vertical sleeve gastrectomy ) is a procedure in which about ¾ of the stomach is removed leaving a narrow gastric tube or “sleeve” through which food passes. The removed part of the stomach includes fundus; which is the balloon like upper part of stomach which easily stretches with food. Stomach Fundus is also important as it releases hormone Ghrelin .This hormone is termed as ‘hunger hormone’ because it stimulates appetite, increases food intake and promotes fat storage. Due to this small stomach tube, the amount of food ingested is restricted and a person can take small amount of food at a time thereby the amount of calories consumed is restricted which results in weight loss.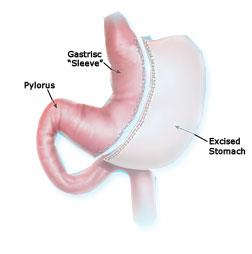
The Surgery does not involve any procedures on intestine ; therefore food malabsorption does not happen with Sleeve Gastrectomy.
Apart from the restriction to food and reducing the hunger feeling this surgery causes rapid transit of food in proximal small bowel which has an important role in controlling disease like diabetes. Sleeve Gastrectomy alone is regarded today as a powerful weight loss operation where the weight reduction achieved over 2 years is comparable for most by pass procedures.
As the fundus or the “ballooning” part of stomach is removed the stomach becomes a “high pressure” tube after this procedure and some degree of reflux is seen in many patients. Therefore it has to be performed with caution on patients who already have acid reflux disease. Staple line leaks can occur in about 2-3% of patients which often can be managed with non surgical methods. If weight gain occur after several years following surgery it can easily be converted to several types of bypass procedures.
This is the longest standing or “Gold standard” Bariatric surgical procedure where the outcomes of other bariatric surgical procedures are often compared with. In this operation a 20-30 cc gastric pouch is created just below the Gastro-Oesophageal junction which essentially functions as a small stomach. Thereafter the proximal small bowel (jejunum) is divided at about 150-200cm from Duodenum and is being brought up and connected to the gastric pouch to form the “food” limb. The remaining end of the proximal jejunum is connected to this further down as a bilio-Pancreatic limb to complete the operation.
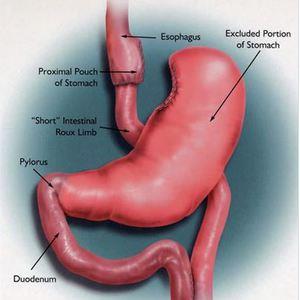
Whilst providing restriction to food intake this operation effectively bypasses about 1/3rd of the effective nutrient absorbing area of small bowel causing “mal-absorption” leading to rapid weight reduction and control of illnesses associated with obesity.
Anastamotic leaks and weight gain after a time period can occur with this procedure. Internal hernia related to small bowel with weight loss is also a known complication of this surgery.
This relatively novel operation is rapidly gaining popularity in Asian countries due to its ability to rapidly control obesity associated illnesses like diabetes and fatty liver disease. This operation includes a sleeved stomach (where the remaining stomach is left intact unlike in sleeve gastrectomy) and by pass of 150-200cm of proximal small bowel with a single anastomosis (joint) to the gastric tube ; giving it both a restrictive and a malabsorptive mechanism of action.
The issue of “high pressure stomach” in Sleeve Gastrectomy is resolved with this operation ‘ giving the patient more “freedom” with regard to consuming food. However if unhealthy food is consumed the patient can develop “cramps” and diarrohea due to malabsorption and bile reflux also can be troublesome to a few patients which is often transient.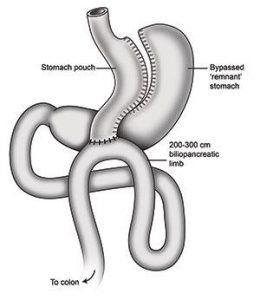
This operation can easily be converted to another bariatric operation in the event of an acute complication. Also if long term malnutrition occurs 50% of the surgery can easily be reversed with a simple laparoscopic technique.